|
Prevalence and Prevention of ACL Injuries in Female
Athletes
|
Written by:
|
Reviewed for medical accuracy by:
|
Added to knowledge base:
|
|
Karen Kinnaman
|
|
01/08/07
|
|
UM
Medical School
|
|
|
|
|
|
Since the passing of Title IX of the Education Amendments of
1972, which sought equity for girls and women in sports, female participation
in athletics has increased dramatically. In high school, participation
has skyrocketed from 294,015 in 1971 to 2,472,043 in 1997, while in college;
participation has more than tripled, from 31,000 to 128,208.1 As
more and more females take to the courts and fields to partake in intense,
physical play, so has increased the incidence of injuries, especially those to
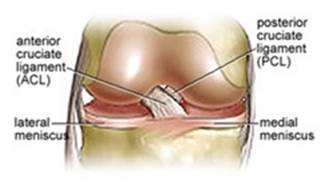
the Anterior Cruciate Ligament or ACL. The ACL is a ligament located
inside the knee which functions to prevent to the tibia (shin bone) from
sliding forward, prevent hyperextension of the knee, and stabilize the knee
during twisting motion. When one engages in such activities as biking
or swimming, there is minimal stress to the ACL as little twisting is
involved. In sports that require planting, cutting, and explosive
changes in direction, like soccer, skiing, and basketball, the ACL plays a
crucial role and is therefore the target of many sprains and tears.
Studies have shown that female athletes are two to eight times more likely to
injure their ACL than male athletes depending on the sport and level of
competition.2 Many of these injuries are occurring in women between the
ages 15 and 25. Although the exact reasoning for the higher incidence
of ACL injuries in female athletes is unclear, studies have suggested the
discrepancy to be the result of hormonal, anatomical, and biomechanical
differences.
Hormones
A study in 1998 on the impact of hormones on ACL injuries in female athletes
revealed that more ACL injuries occurred than expected during the ovulatory
phase of the menstrual cycle when estrogen levels are high as compared to the
luteal and follicular phase.2 Estrogen or progesterone’s direct
effect on collagen metabolism could affect the strength of the ACL and
predispose women to a higher risk of injury.2 Liu et al found that
there are estrogen and progesterone receptors on the ACL.11 Current studies
are evaluating whether those in ovulatory cycles are at higher risk of injury
than those who are non-ovulatory or taking oral contraceptive pills, and
whether hormones may have an effect on reaction time.
Anatomy
Although it has not been completely determined, some studies have shown that
the groove through which the ACL travels, called the intercondylar notch,
tends to be narrower in women as compared to men, leading to a higher
incidence of ACL injuries.3 As the ACL moves within this notch, it provides
stability to the knee and prevents the tibia from both moving too far forward
and rotating too far inward. A narrower intercondylar notch, as seen in
women, can limit the space for ACL movement, causing the ACL to pinch more
easily as the knee bends during twisting and hyperextension movement.
Such pinching of the ACL can lead to rupture or tear.
Additionally, women have a wider pelvis then men, making the thigh bones
angle more sharply as they connect to the shin bone. As this “Q
angle” increases due to wider hips, greater pressure is placed on the
ACL ligament as the knee twists.
Biomechanics
Research has shown that biomechanical factors such as joint forces and
landing technique, muscle activation patterns, and muscle strength imbalances
may be the biggest contributors to the increased risk of these injuries among
females. Dynamic stability is related to quadriceps and hamstring
action at the knee. While men fire their hamstring muscles first for
pivoting or landing from a jump, female athletes fire their quadriceps muscle
first. Contraction of the quadriceps can pull the tibia forward,
increasing the strain on the ACL and risk for rupture.5 Studies suggest
that the hamstring muscles assist the ACL by reducing the forward motion of
the tibia induced by the quadriceps.6 The imbalance between quadriceps
strength and hamstring strength seen in female athletes after menarche puts
them at greater risk for ACL injuries.7 Many also believe that coaching
plays a role in women’s increased risk for injury, as women tend to
land from a jump in a riskier position (angle at the hip and knee).12
It has been shown, as noted below, that women can be taught to land
differently, which has been shown to reduce the risk of injury.
These biomechanical findings have led to the development of
ACL injury–prevention programs that work to improve the dynamic control
of the knee by emphasizing hamstring strengthening, landing technique, and
proprioception. Studies indicate that these “jump training
programs” can reduce risk of ACL injury up to 80%.
How to
Prevent ACL Injuries
Approximately 80% of ACL injuries are due to non-contact events such as a
sudden stop, change in direction, or landing from a jump.8 Therefore,
as recent studies have suggested, proper strength and conditioning training
to stabilize the muscle around the knee can prevent such injuries. One
such training regime, the PEP (Prevent injury, Enhance Performance) program,
was developed for female soccer players by Dr. Bert Mandelbaum of the Santa
Monica Orthopedic and Sports Medicine Group. The 15-minute-a-day
program, performed 2-3 times a week, focuses on avoiding vulnerable
positions, increasing flexibility, strengthening major muscle groups,
learning to land correctly with a bent knee and hip, increasing
proprioception through agility drills, and engaging in plyometrics. In
a two-year clinical prevention trial among 1,400 NCAA Division I female
soccer players, 52 teams participated in the PEP program for a total of 12
weeks. Two ACL tears were reported on the teams that implemented the
PEP program as compared to 32 tears among athletes in the control group on
teams that did not implement the program. These results demonstrated
that increased strength, proprioception, flexibility, and agility can reduce
by up to 88 percent non-contact ACL tears in female athletes.9
A sample PEP program includes:
- Warm-ups: Jog, slides, backpedals
- Stretching: Hamstrings, quadriceps, calves, groin and
hip flexors
- Strengthening: Lunge walk, Russian hamstring, toe
raise
- Plyometrics: Lateral, front/back, and single leg
hops; vertical and scissor jumps,
- Agility: Shuttle and pivot runs
Education about the increased risks of ACL injuries among
female athletes should be used in a way to prevent such injuries, not used to
discourage female participation in athletics. There are variations of
ACL prevention programs available on the Internet aside from the PEP program,
and athletes should seek a strength and training program that works to
improve upon their own weaknesses. When looking for a program suitable
for the individual, one should look for a regime that focuses on enhancing
control of muscles throughout the legs, establishing good hamstring to
quadriceps ratios, and developing good proprioceptive skills. As female
athletes continue to advance women’s sports to even more competitive
and intense levels, the threat of injury becomes more prevalent, as more than
30,000 high school and college age females are expected to rupture their ACL
each year.10 Additionally, osteoarthritis of the knee has been
found to occurs at a 10 times greater rate in ACL-injured patients, regardless
of whether the injury is surgically or non-surgically treated.13Therefore,
preventive efforts should be taken in order to avoid such debilitating ACL
injuries in order to allow for continued dominance in the athletic
forum.
1. “Title IX
Q&A”. May 26, 2005. /cgiin/iowa/issues/rights/article.html?record=888
2. Edward M. Wojtys, Laura J. Huston, Thomas N.
Lindenfeld, Timothy E. Hewett, and Mary Lou V. H. Greenfield. Association
Between the Menstrual Cycle and Anterior Cruciate Ligament Injuries in Female
Athletes. Am.
J. Sports Med., Sep 1998; 26: 614 - 619.
3. RF
LaPrade, QM Burnett. Femoral intercondylar
notch stenosis and correlation to anterior cruciate ligament injuries. A
prospective study. Am
J Sports Med. 1994
Mar-Apr;22(2):198-202.
4. Jamie L. Moul, EdD, ATC. Differences in Selected
Predictors of Anterior Cruciate Ligament Tears Between Male and Female NCAA
Division I Collegiate Basketball Players. J Athl Train. 1998 Apr;33(2):118-121.
5. Beynnon B, Howe JG, Pope MH, Johnson RJ, Fleming BC.
The measurement of anterior cruciate ligament strain in vivo. Int Orthop. 1992;16:1–12
6. Baratta R, Solomonow M, Zhou BH, Letson D, Chuinard R,
D’Ambrosia R. Muscular coactivation: the role of the antagonist
musculature in maintaining knee stability. Am J Sports Med.
1988;16: 113–122
7. Christopher
S. Ahmad, MD, A. Martin Clark, MD, Niels Heilmann, J. Scott Schoeb, MD,
Thomas R. Gardner, PE and William N. Levine. Effect of Gender and Maturity on Quadriceps-to-Hamstring
Strength Ratio and Anterior Cruciate Ligament Laxity. Am J Sports Med. 2006 Mar;34(3):370-4.
8. Griffin LY, Agel J, Albohm MJ, Arendt EA, Dick RW,
Garrett WE, Garrick JG, Hewett TE, Huston L, Ireland ML, Johnson RJ, Kibler
WB, Lephart S, Lewis JL, Lindenfeld TN, Mandelbaum BR, Marchak P, Teitz CC,
Wojtys EM. Noncontact anterior cruciate ligament injuries: risk factors and
prevention strategies. J
Am Acad Orthop Surg. 2000 May-Jun;8(3):141-50.
9.Silvers HJ, Giza ER, Mandelbaum BR. .Anterior cruciate ligament
tear prevention in the female athlete.. Curr Sports Med Rep.2005
Dec;4(6):341-3.
10. “University Sports Medicine Brings ACL
Injury Prevention Program to Rochester: Research Shows Program Can Reduce Risk of Injury by 90
Percent.” December 17, 2003.
11. Lui, X., Luo ZP. Combined effects of estrogen
and mechanical loading on anterior cruciate ligament fibroblast
biosynthesis. Scientific World Journal 2005 Jan 14;5:5-8.
12. Hewett TE, Lindenfeld TN, Riccobene JV, Noyes
FR. The effect of neuromuscular training on the incidence of knee injury in
female athletes: a prospective study. Am J Sports Med.
1999;27:699–706.
13. Fleming BC. Biomechanics
of the anterior cruciate ligament. J
Orthop Sports Phys Ther. 2003;33:A13–A15.
|
|


